

Abstract
BACKGROUND: Fat Embolism Syndrome (FES) is common in trauma patients and those with long bone fractures. It can also be a rare complication of bone marrow necrosis (BMN) in patients with sickle cell hemoglobinopathies (SC), particularly HbSβ+ and HbSC, due to marrow ischemia resulting from sickling with subsequent hematopoietic and stromal cell death. Release of intramedullary fat emboli causes multiorgan failure with anemia and thrombocytopenia, often mimicking TTP. Here, we discuss the clinical presentation and outcomes of 16 patients with SC and FES, and attempt to distinguish it from TTP.
METHODS: We compared SC patients with FES treated at our institution between April, 2010 and January, 2018 with 2 TTP patients matched for age, gender and race. We analyzed their presenting symptoms and labs aiming at identifying characteristics that differentiate the two conditions. A univariate exact conditional logistic regression was used to examine significant differences in likelihood of FES for continuous and categorical variables. A Friedman test was used to test for significant differences in schistocytes on admission. Ordinal values were created based off the value of the dependent variable, i.e., presence of schistocytes (none=0, rare=1, few=2, occasional=3, moderate=4, and many=5/high power field). This test accounts for the 1:2 matching and the null hypothesis is that there is no difference in ranks by patient group. The study was approved by our Institutional Review Board.
RESULTS: Sixteen patients with SC (10 with HbSβ+, 4 with HbSC and 2 with HbSS disease) were treated for FES at our institution, mean age 40.6y. At presentation, 11 (69%) complained of severe back pain, 11 (69%) had respiratory compromise, and 9 (56%) had altered mental status. On admission, all patients were anemic, with a mean hemoglobin of 9.2 g/dL. Thrombocytopenia was present in 12 patients (75%) at admission, and the rest developed it during the hospitalization. Six (38%) patients had a leukoerythroblastic picture on admission with >20 nucleated RBC/ 100 leukocytes, and another 7 (total, 81%) developed it later. Of the 10 patients who had ferritin measured, all had an increased level (mean 5792 ng/mL; ref: 10-291 ng/mL). Of the 12 patients who received RBC transfusion (10 exchange and 2 simple transfusion), 9 had full recovery, 2 had neurologic impairment and 1 died. Those with delayed recognition of FES either died (n=3) or suffered permanent neurologic damage (n=1).
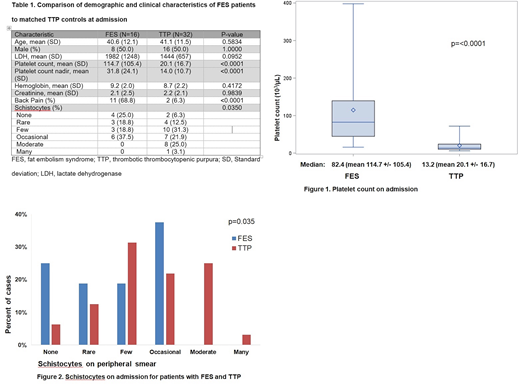
Table 1 compares the clinical characteristics of the SC patients who developed FES with matched TTP patients. The latter had significantly lower platelet count on admission and at nadir during their hospital-stay compared to FES patients (p<0.0001) (Fig 1). Also, back pain was reported significantly more in patients with FES (p<0.0001). Indices on admission that were not significantly different between the two groups included hemoglobin, lactate dehydrogenase, creatinine, or a leukoerythroblastic pattern on peripheral smear. FES patients were less likely to have moderate/many schistocytes on peripheral smear compared to TTP patients (p=0.035) (Fig 2).
DISCUSSION: BMN and embolization of fat and necrotic marrow is a rare but potentially fatal complication in SC patients. It can be the first manifestation of SC disease in previously undiagnosed patients, leading to delayed diagnosis. In several published fatal cases of BMN, the diagnosis was only made at autopsy. The etiology and precipitating factors of BMN/FES remain poorly understood, though association with Parvovirus infection has been reported. In the past 8 years, we have diagnosed 16 patients with FES, who presented with an array of nonspecific symptoms such as fatigue, mental status changes, bone pain, fever, anemia, thrombocytopenia, and leukoerythroblastic picture in the peripheral blood. Since FES and TTP have similar clinical and laboratory features, identifying early signs that differentiate the two is essential for optimal treatment and survival. While both disorders have mortality approaching 90% if untreated, therapeutic plasma exchange is life-saving in TTP, and patients with FES appear to benefit from red cell exchange. Increasing awareness of hematologists, maintaining a high index of suspicion for FES, establishing the correct diagnosis early, and instituting rapid intervention with red cell exchange or simple transfusion is essential to prevent permanent dysfunction or death.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal